Rethinking the Alar-Base Reduction: When, How, and Why to Reduce the Nostrils in Rhinoplasty
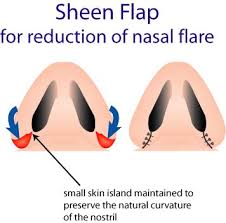
Reducing nostrils is an oftentimes major goal in rhinoplasty, particularly for ethnic noses but can be so for any ethnicity. There are many considerations when discussing this topic of alar-base reduction. The first is the importance of preserving the nostril shape and the nostril sill. Too often you see cut off nostrils where the shape of the nostril has been severely compromised, and the Jackson family is perhaps the worst public case of this and I mean all of them, LaToya, Janet, and the deceased poster boy of bad rhinoplasty, Michael Jackson. The cut-off nostril appearance is due to the old Weir-type incision in which the nostril sill (like a window sill that sits between the nostril and the upper lip) has been amputated and the shape of the nostril looks cut off. What I do to avoid this problem is to use a combination of two maneuvers. First, I perform what is known as a Sheen flap, so I don’t violate the nostril but stay outside of the nostril right up to about a millimeter of tissue. This preserves the natural curvature of the nostril. What the Sheen flap accomplishes is the reduction in the nostril flare but it doesn’t actually reduce the nostril size. I then perform, as needed, a nasal sill reduction, where I remove along the straight nasal sill a portion of it to shrink the nostril. By separating the nostril into a nasal sill reduction and an outer Sheen flap alar-base reduction, I can accomplish both goals while preserving the natural shape of the nostril.
The next fear of an alar-base reduction is unfavorable scarring. What I have found is that the transcolumellar incision (between the nostrils) used to perform a standard open rhinoplasty heals tremendously well. However, the alar-base reduction can heal unfavorably, not a keloid but just unfavorably where you can see the incision if you are relatively close up. Even though my transcolumellar incisions have healed tremendously well, in the past 3 years they have healed even better because I learned in St. Petersburg, Russia, where I was lecturing to use a dissolvable suture during that conference. I have now moved that knowledge over to my technique for alar-base reduction and have noticed a similar tremendous improvement. Regardless, I am always more careful in letting my patients know if they undergo an alar-base reduction that they may require a few steroid/5-fluorouracil (scar dissolver) injections and possibly dermabrasion as well to make the incision as flawless as possible.
Another important point is that I don’t just knee-jerk reduce the alar base. The reason for my caution is that sometimes the central nasal tip is very broad and can only be reduced so much. Given that constraint, you do not want to reduce the sides too much, or sometimes not at all, because it can make the central tip look even fatter. This balance in size between the central nasal tip, the nasal sides, and the nasal bridge is a critical element to good rhinoplasty and requires artistic judgment from the rhinoplasty surgeon to decide the best relative proportion for each part of the nose.